Currently, some of the reproductive health treatment options include hormonal stimulation, intrauterine insemination, In Vitro Fertilisation (IVF) or Intracytoplasmic Sperm Injection (ICSI), gamete donation, and uterine surrogacy. In both sexes that experience reproductive health problems, treatment options depend on the assertion that both partners produce functional gametes. In couples where one partner is unable to produce functional gametes, no treatment possibilities are currently available other than the use of donor sperm or eggs. Genetic syndromes and medical treatments such as chemo- or radiotherapy and immunosuppressive treatments are the most common reasons for the absence of functional gametes. Many couples struggle with this since there is no full genetic link with the child. Various alternatives to produce functional gametes have been suggested by using germline progenitors, or patient-specific or umbilical cord tissue pluripotent stem cell-derived gametes (3, 4).
Research in stem cells and regenerative medicine is on the increase with promising clinical trials in the initial stages. The specific potency, self-renewal, and tissue repair features of stem cells have great possibilities for the treatment of male and female reproductive health problems and have been used in research and treatment of various of these diseases. Various types of stem cells, including adipose stem cells, bone marrow stem cells, and umbilical cord stem cells are being tested in clinical trials for the treatment of reproductive health problems. These stem cells have shown positive results in improving the “microenvironment”, repairing the function of reproductive organs, forming germline stem cells, and thereby improving reproductive capacity directly.
Figure: Potential applications of Stem cells on various reproductive diseases.
For stem cell therapy to progress, there needs to be further long-term planning, strict evaluation, and supervision to ensure the accuracy, quality, and safety of the use of stem cells in this field. Since the patient’s own stem cells and recently the use of umbilical-derived stem cells are more ethical, safe, and non-immune, the use of these types of stem cells will more likely be used in the future treatment of reproductive health problems.
There is however a cautionary note to couples: There are untested therapies where stem cells are used to treat reproductive health problems. Therefore, please consult with your reproductive physician to understand both the challenges and possibilities of solving reproductive health problems in the future.
In 2016 the Fred Hutchinson Cancer Research Centre, in the United States, reported from a review done in patients they compared outcomes after receipt of a transplant from a cord-blood donor with outcomes, after receipt of a transplant from an HLA-matched or HLA-mismatched unrelated donor in patients with acute leukemia or the myelodysplastic syndrome who underwent a first myeloablative allogeneic transplantation. All patients with acute myeloid or lymphoid leukemia or myelodysplastic syndrome who received a first allogeneic hematopoietic-cell transplant from an unrelated donor between January 2006 and December 2014 (582 patients), with the source of stem cells being cord blood, bone marrow, or peripheral blood. All cord-blood grafts were matched for four, five, or six loci at HLA-A and HLA-B (at the antigen level) and at the allele level for HLA-DRB1. In the unrelated-donor groups, which included bone marrow and peripheral-blood stem-cell sources from adult volunteer donors, patients were matched with the donor at the allele level for HLA-A, HLA-B, HLA-C, HLA-DQB1, and HLA-DRB1 (HLA-matched group) or were mismatched for a single allele (HLA-mismatched group). In the HLA-matched and HLA-mismatched groups, the stem-cell source was determined largely according to treatment protocol and in some cases according to donor or patient preference. HLA-matched unrelated donors were generally selected as the primary source if patients did not have an HLA-matched related donor.
These results showed that in patients with minimal residual disease, the use of cord blood as the donor source for hematopoietic-cell transplantation led to a higher rate of survival and a lower rate of relapse than the use of a transplant from an HLA-mismatched unrelated donor.
Another similar review of the literature was done by another major cancer centre in the United Kingdom comparing transplants from various children’s cancer hospitals in England in 2023. This review, similar to the United States study, found that in patients at high risk of relapse after transplant, cord blood transplant recipients have better survival outcomes when they have high-risk and relapsed/refractory paediatric myeloid malignancy (1-3).
The United States study reviewed outcomes for 582 patients who received stem cell transplants from 2006, until 2014. Of those, 140 patients received cord blood transplants. In the United Kingdom study, a review of 367 patients received transplants; of these 112 patients received cord blood transplants, whilst 255 received transplants from other sources, between January 2014 and December 2021. Both these studies concluded that patients that received a cord blood transplant had better survival and less relapse than patients that received stem cells from adult, unrelated donors.
Cord blood transplantation has been associated with less chronic graft-versus-host disease (GVHD) and “could enable nearly all patients to have an available donor”. On the other hand, haploidentical cord transplants are being used increasingly, even in older patients, and maybe another alternative for better outcomes. In addition, the expansion of cord blood provides another level of availability for paediatric and adult patients that require an urgent transplant.
In a large, retrospective registry study of Japanese adult patients with non-remission AML, the relapse rate was reduced in cord blood stem cell transplant recipients compared with matched family donors, and their disease-free survival was better. The low incidence of chronic GvHD combined with the Graft-versus-leukemia effect that cord blood affords has also resulted in superior chronic GvHD-free relapse-free survival (GFRFS) for cord blood compared with other donor sources in further studies (4).
All three of these studies, therefore, highlight and show that currently, if patients have high-risk disease and are at high risk for relapse post-transplant, a transplant with a cord blood donor may be the best option.
Immunotherapy, a type of treatment that activates a patient’s immune system to target cancer cells, has been successful in many diseases but not ovarian cancer and it is unclear why. Adoptive cell therapy is a rapidly expanding approach to cancer immunotherapy to facilitate antitumour reactions by introducing potent effector cells into the tumour microenvironment. In this context, neutrophils, and natural killer cells as a substantial proportion of the innate immune system have been reported to exert anti-tumourigenic roles in the tumour microenvironment.
How do Neutrophils and Natural Killer Cells work?
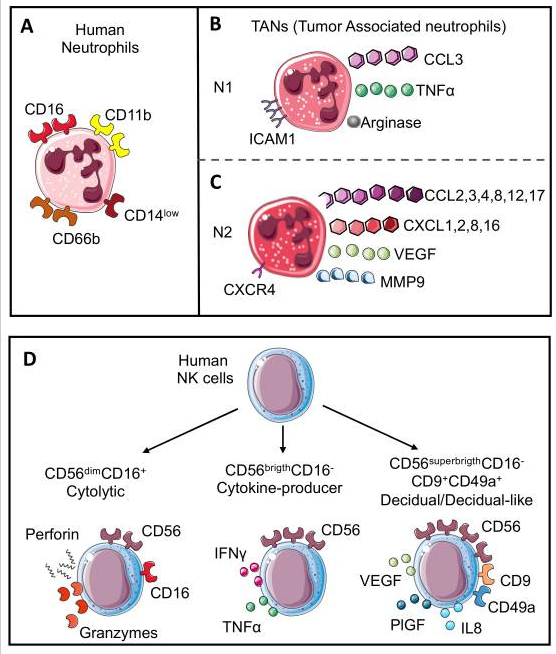
Neutrophils are the most abundant circulating leukocytes, accounting for 50–70% of blood cells. During neutrophil maturation from common myeloid progenitors, the granulocyte-monocyte progenitor cells are the first to acquire the neutrophil lineage marker CD66b. Then, during maturation, from promyelocytes to human mature neutrophils, the simultaneous acquisition of CD11b and CD16 can be observed (Figure 1).
Fig. 1: Neutrophil and NK cell subsets
Human neutrophils (A) are characterized by CD11b, polarization, neutrophils in the tumour microenvironment are also characterized by the capability to acquire two opposite phenotypes. N1 neutrophils (B) show antitumoural activities and are characterized by the expression of chemokine (C-C motif) ligand 3 (CCL3), tumour necrosis factor α (TNFα), arginase, and intercellular adhesion molecule 1 (ICAM1); in contrast, N2 neutrophils (C) work as tumour-promoters and express CC and CXC chemokines (CCL2, 3, 4, 8, 12 and 17 and CXCL1, 2, 8, and 16), vascular endothelial growth factor (VEGF), matrix metalloprotease 9 (MMP9), and CXCR4 receptor. Human NK cell subsets (D) are characterized by CD56 expression. Cytolytic NK cells express CD56 and CD16 (CD56dimCD16+) and can release perforin and granzyme; cytokine-producer NK cells lose CD16 expression and increase CD56 expression (CD56brigthCD16−) with the production of cytokines including TNFα and interferon γ (IFNγ); the last subset is named decidual cells (dNKs) that displayed higher expression of CD56 with CD9 and CD49a markers (CD56superbrigthCD16−CD9+CD49a+) and support angiogenesis through the release of VEGF, placental growth factor (PlGF), and interleukin 6 (IL6). A similar subset named decidual-like NK cells is also found in the tumour microenvironment (TME).
Neutrophils represent the first-line defence against infections, thus they are rapidly recruited from the bloodstream to the site of injury where they eliminate pathogens, particularly bacteria, by phagocytosis, degranulation, and release of extracellular traps (NETs).
In both macrophages and neutrophils opposite functions or heterogeneity has been described, and the existence of opposing polarization states (pro-tumoural or anti-tumoural) of macrophages and neutrophils in cancer. In cancer, mimicking the dichotomy between proinflammatory/ M1-like and anti-inflammatory/tissue-repairing/TAM/M2-like macrophages, neutrophils have been conventionally termed N1 and N2 neutrophils, with the latter characterized by immunosuppressive, pro-metastatic, and pro-angiogenic activities.
Natural killer (NK) cells are large granular lymphocytes from innate immunity, participating in the early recognition and elimination of virus-infected and malignant-transformed cells. Currently, NK cells are classified as innate lymphoid cells (ILCs) and originate from common innate lymphoid progenitors in the bone marrow. Subsequently, they migrate to different lymphoid tissues or non-lymphoid tissues, where they are “educated”, acquiring phenotype and functions typical of tissue residency. The NK inhibitory receptor repertoire is adapted to the MHC class I molecules borne by the host, assuring NK cell tolerance against self-cells. On the other hand, NK cells are simultaneously stimulated by activating receptors that trigger NK cell responses. In the presence of healthy cells, activating signals are low, thus the binding of inhibitory receptors to MHC class I molecules is sufficient to induce NK cell tolerance. In contrast, when NK cells recognize altered cells (i.e., tumour cells) that lack or downregulate MHC I expression, the activating signals overcome the inhibitory ones, leading to the killing of altered cells.
Fig. 2: Neutrophil–NK cell crosstalk in tumour microenvironment
Neutrophils can (A) induce a reduction in CCR1 expression in NK cells, impairing the NK cells’ infiltration capability. Interference with PDL1-PD1 (B) interactions in the TME, resulting in reduced NK cell capability to release IFNγ. Neutrophils can also modulate the expression of activating receptor NKp46 on NK cells through (C) the release of different molecules that include: (i) neutrophil-derived Cathepsin G (CG) reduces NKp46 on NK cells; similar; (ii) reactive oxygen species (ROS) can downmodulate NKp46 on cytotoxic CD56dimCD16+NK cells while they can upregulate this receptor on cytokine-producer CD56brigthCD16− NK cells; (iii) elastase and lactoferrin release exerts a wide effect increasing cytotoxicity and reducing angiogenesis. NK-derived IFNγ, a key mediator in TME, can be inversely modulated by ARG1 and IL12 from neutrophils (D). (i) Indeed, neutrophil-derived ARG1 can abrogate IFNγ released from NK, improving NK pro-angiogenic features; (ii) while neutrophil-derived IL12 through STAT4 activation increases IFNγ and perforin production by NK cells. NK cell–neutrophil crosstalk (E) can be modulated by NK-derived IFNγ, which acts by decreasing pro-angiogenic features of tumour-associated neutrophils (TANs). Indeed, NK cells or IFNγ depletion increase TANs’ pro-angiogenic features. (1)
Tumour-associated neutrophils have been shown to robustly produce a variety of toxic compounds and can induce tumour cell cytolysis or cytostasis in vitro, which suggests that in certain circumstances they might oppose tumourigenesis. The mechanisms of neutrophils killing cancer cells may be direct cytotoxicity toward tumour cells. Neutrophils can be polarized into different phenotypes according to various cytokines secreted by cancer cells in the tumour microenvironment.
Focus on Immunotherapy, mesenchymal stem cells and stem cell secreted factors
The current focus of research on ovarian is to improve our understanding of the immune environment in ovarian cancer in hopes of making immunotherapy an option for these patients. Recent evidence has pointed to key characteristics of immune cells in ovarian cancer and identified cell types important for mediating an immune response.
To obtain an adoptive cell therapy (ACT) exploiting allogeneic neutrophils which are easily available and abundant; umbilical cord blood-derived neutrophils offer superior amounts over other sources of neutrophils. For example, researchers have shown that LPS and IL-8-activated neutrophils from umbilical cord blood (UCB) could inhibit the progression of ovarian cancer cells. Thus, providing strong evidence of UCB-derived neutrophil-based immunotherapy against ovarian cancer (2-3).
Various ovarian cancer xenograft models have been established to evaluate the efficacy of NK cells. Data to support this is provided; for example, SR1/IL–15/IL12 expanded UCB-NK cells constitute a promising immunotherapeutic product that can be exploited for intraperitoneal therapy of ovarian cancer patients, as demonstrated by their capability to actively migrate, infiltrate, and mediate intra-tumoural cell killing in OC spheroids. In addition, promising preclinical anti-ovarian cancer activity of UCB-NK cells was also demonstrated following intraperitoneal infusion in a relevant SKOV-3-based ovarian cancer xenograft model (4-5).
Premature ovarian insufficiency (POI) and infertility are common and severe side effects of chemotherapy. Chemotherapeutic agents target oocytes directly or induce oocyte death indirectly by damaging somatic cells.
Recently, stem cell transplantation has been shown to be a new strategy for the treatment of POI and infertility following chemotherapy. Based on the evidence, stem cells enhance ovarian function due to their paracrine effects rather than differentiating into specific cells. Studies on stem cell-derived secreted factors show that the secretome, microvesicles, and exosome are all found in the medium where stem cells were cultured, which is known as conditioned medium (CM). The contents of these vesicles secreted by mesenchymal stem cells (MSCs) include cytokines and growth factors, signalling lipids, messenger RNAs (mRNAs), and regulatory miRNAs. These factors are involved in cell–cell communication, cell signalling, and alteration of cell or tissue metabolism. CM could promote tissue/organ repair under various conditions. In addition, CM has several advantages compared with stem cells. (i) CM can be manufactured, freeze-dried, packaged, and transported more easily, (ii) it eliminates issues with matching the donor and the recipient to avoid rejection problems; and (iii) it eliminates the potential side effects of stem cells on tumour cells, such as differentiating into other stromal cell types, increasing the metastatic abilities of tumour cells, and stimulating the epithelial–mesenchymal transition of tumour cells.
In addition, recent studies showed that Human umbilical cord mesenchymal stem cell (hUCMSC) transplantation can reduce cumulus cell apoptosis, and restore ovarian function. Even primordial follicles in the ovaries treated with hUCMSC-CM exhibited an apparent resistance to cisplatin. Additionally, ovarian reserve and fertility can also be preserved after hUCMSC-CM treatment. CM derived from human amniotic epithelial cells (hAECs) can protect ovaries against chemotherapy-induced damage and 109 cytokines in hAEC-CM might participate in apoptosis, angiogenesis, cell cycle, and immune response.
In conclusion, the value of hUCMSCs to exert protective effects on cisplatin-induced ovarian damage via the paracrine pathway has clearly been demonstrated. These results will add value in promoting the application of CM in clinical treatment, and hopefully, infertile patients can benefit from hUCMSC-CM treatment in the future (7-18).
All the above results demonstrate that ovarian cancer, despite resistance to existing immunotherapies, is indeed an immunogenic disease and provide a roadmap for the design of improved immunotherapy options by using allogeneic stem cell-based therapies, which could even be applicable to other tumours with similar mutational burden.
In addition, MSCs cells are easily accessible, do not induce immunological responses, can be simply manipulated in vitro without the requirement for immortalization; can preferentially migrate into the tumour tissues and have transactions with various cells in the tumour microenvironment. MSCs therefore, are the most appropriate choices for cell-based treatments in cancers. Notwithstanding, the progress in obtaining enough autologous and allogeneic MSCs from bone marrow, adipose tissue, umbilical cord blood, and local tissues, however, their mechanisms of action still require further investigation. Additionally, exosomes released by MSCs and their manipulation may offer another promising technique in MSC-based cancer therapy. Despite providing a novel and attractive therapeutic system in cancer therapy, MSCs have been accompanied by several challenging issues and limitations.
Thus, future clinical trials to evaluate the efficacy of immunotherapy and MSC-based treatment strategies in ovarian cancer might prove imperative in the battle against this fatal gynaecological malignancy.
Insistent infection of the cervical epithelium by high-risk HPV can lead to cervical intraepithelial neoplasia which may progress to invasive cervical cancer, such as squamous cell carcinoma, adenosquamous cell carcinoma, or adenocarcinoma. The most conventional treatment for earlystage cervical cancers is radical hysterectomy (surgical removal of the cervix, uterus, and surrounding tissues called the parametrium) (2).
The alternative is radiation therapy (RT), which is usually given in combination with chemotherapy. In advanced (metastatic) diseases, targeted therapies are widely explored. Regrettably, limited success has been achieved using targeted intervention strategies with small molecules, angiogenesis inhibitors, and monoclonal antibodies directed against specific tumour antigens and proliferation pathways. For example, overexpression of EGFR has been linked with poor prognosis in cervical cancer, thus EGFR is an ideal candidate for therapeutic targeting. However, even limited success has been achieved with monoclonal therapy using cetuximab (CET) (chimeric IgG1, anti-EGFR mAb) as monotherapy or CET in combination with chemotherapy.
An alternative therapy has been the use of immunotherapy for cervical cancer. Even this has shown limited success. The focus of this has been vaccination approaches against HPV-derived oncogenes (E6 and E7) to trigger an efficient antitumor T cell response. These failed responses have been contributed to the extensive HLA down-regulation commonly observed in cervical cancer. Thus, it is believed that natural killer (NK) cell-based therapies may prove more effective than T cellbased approaches in the treatment of cervical cancer. The role of the innate immune response in host defense and viral clearance during (early) infection is well recognised. NK cells are potent in exerting rapid cytotoxicity by releasing cytotoxic granzyme B and perforin to lyse virus-infected cells and tumour cell targets. The efficient activity of NK cells is regulated by an equilibrium between inhibitory (e.g., CD94/NKG2A) and activating (e.g., CD16, DNAM-1, CD94/NKG2C, CD94/NKG2D) receptors. Various strategies have been adopted to cure cancer, such as adoptive cellular immunotherapy, including chimeric antigen receptors (CARs)-T cells-based and natural killer (NK) cell-based therapies. These therapies have made substantial improvements in the prognosis of patients.
NK cells are the core cells of the innate immune system and are the first line of defense against cancer cells and virus infection. NK cells can kill tumour cells without antigen sensitisation and antibody involvement. In recent years they have been used in the immunotherapy of malignant tumours. NK cells use unique mechanisms that depend on a set of stimulatory and inhibitory receptors, such as NKp30, NKp46, NKG2D, and NKG2A, and these receptors, function as switches, to determine whether NK cells are activated to kill target cells. Once activated, NK cells release perforin and granzyme; perforin perforates the surface of target cells, facilitating granzyme B to induce the apoptosis of target cells. In addition, NK cells can also secrete amounts of cytokines, including IFN-γ and TNF-α, which act on the target cells directly or further activate other types of immune cells. Another activation mechanism of NK cells is to enable target cells to be programmed for apoptosis through Fas/FasL or TRAIL (3).
NK cells can be derived from various sources, including umbilical cord blood (UCB), induced pluripotent stem cells, peripheral blood (PB), and embryonic stem cells. Unlike PB, UCBs are easy, quick, and pain-free to collect at birth and cryopreserved, making them readily obtainable. Of note, UCB has also been regarded as an allogeneic and off-the-shelf source of NK cells. Various expansion methods have been exploited to elevate the number and activity of NK cells to satisfy clinical use. Given that preclinical and clinical results of UCB-derived NK cells-based therapies have shown positive outcomes, it is reasonable to conclude that this form of immunotherapy is attractive and promising.
Although unexpanded UCB-derived NK cells have some limitations, including availability in low numbers due to the small volume of the UCB unit and immature function. These shortcomings have been overcome by a diverse range of approaches to expand UCB-derived NK cells in vitro.
To achieve this goal, large-scale expansion in their numbers and enhancing the activity of UCBderived NK cells in vitro were done through a variety of methods. IL-2-alone was previously used to expand NK cell, but this approach did not show significant results and needed further improvement. Subsequently, multiple cytokines-only approaches, including IL-2, IL-12, IL-15, and IL-18, were, therefore, used to satisfactorily expand NK cells. Thus, artificial antigen-presenting cells combined with cytokines have been used to expand NK cells in vitro, with satisfactory purity and number of NK cells (4).
UCB-derived NK cells have demonstrated utility in various clinical applications. Using non-modified UCB-derived NK cells has also shown that UCB CD34+-derived NK cells were more cytotoxic to cervical tumour cells, which were not restricted by HLA-ABC expression, and the levels of degranulation of NK cells were higher, compared to PB-derived-NK cells (5).
Approaches that strengthen the expression of activating receptors or diminish the inhibitory receptors of NK cells have been explored to enhance their activity. For UCB-derived NK cells, the expression of NKG2D in expanded NK cells was elevated in vitro, and NKG2D mediated the cytotoxicity of them against tumour cells. Therefore, the belief is that UCB-derived NK cells can also be genetically modified using CAR (NKG2D-DAP10-CD34), and their cytotoxicity against tumour cells will be enhanced significantly.
Besides, NK cells can also be activated by reducing the expression of inhibitory receptors, such as NKG2A, which can serve as a potential checkpoint for NK cell-based therapy. It is a known fact that the expression of NKG2A is relatively higher in UCB-derived NK cells than in PB-NK cells. Therefore, it would be fascinating to know which of PB or UCB would fare better if antibodies or PEBLs were also used to block the expression of NKG2A. If we speculate; combining UCB-derived NK cells with anti-NKG2A molecules or modifying them with CAR-NKG2A would present much more potent anti-tumour activity than using UCB-derived NK cells only. This aspect has not been studied yet and would provide interesting results in the future.
Only a few studies have investigated UCB-derived NK cells modified via CARs, the results are striking and promising. For instance, NK cells derived from the CD34+ hematopoietic progenitor stem cells of UCB units could be successfully engineered to express CAR-CD19 using co-culture with a feeder stroma of murine OP9-DL1 cells in the presence of human recombinant cytokines. UCB-derived CARCD19-NK cells generated by transducing CAR-CD19 plasmids to UCB-derived NK cells under IL-2 and IL-15 stimulation were more capable of degranulation when co-cultured with CD19 positive cells, compared to non-modified. In the future, except for targeted CD19 antigens, more types of CARs should be gradually engineered into UCB-derived NK cells (6-9).
Thus UCB-derived NK cell-based immunotherapy has boundless therapeutic potential for cancer patients. UCB-derived NK cells’ number and function are typically substantially improved after expansion in vitro. They have the added advantage of possessing high anti-tumour effects both in vivo and in vitro. Therefore, UCB-derived NK cells are a promising allogeneic “off-the-shelf” anti-cancer cellular immunotherapeutic.
Apart from the above-mentioned applications of umbilical cord-derived stem cells, in other studies, umbilical cord mesenchymal stem cells have shown inhibition of cervical cancer. Even exosomal miR-15a-5p from umbilical cord mesenchymal stem cells (UCMSCs) inhibited epithelial-to-mesenchymal transition (EMT) and metastasis of cervical cancer. In other studies, conditioned medium and cellular extract of the human umbilical cord showed inhibition of cervical cancer cells (10-12).
Current pre-clinical and clinical studies have indicated that stem cell-based therapies hold massive potential for the treatment of human disease. Mesenchymal stem cells (MSC) and umbilical cord mesenchymal stem cells in particular are promising anti-cancer agents to treat a number of different cancer types. MSC has inherent “homing” and “tumour-trophic” migratory properties, allowing them to be loaded and to deliver effective, targeted therapy to isolated tumours and metastatic disease. MSC have been readily engineered to express anti-proliferative, pro-apoptotic, anti-angiogenic agents that precisely target different cancer types. Many of these strategies have been validated in a wide range of studies evaluating treatment feasibility or efficacy, as well as establishing methods for real-time monitoring of stem cell migration in vivo for optimal therapy surveillance and accelerated development. Current clinical trials using these stem cells as agents for delivery to various tumour types are underway and hold great promise for novel therapeutic interventions in the future.
Haemophilia A, the most common affects 1 in 10,000 male babies. Clinically, patients with mild deficiency (5–40 % activity of Factor VIII), usually tend to bleed only after major surgical procedures. Patients with moderate deficiency (1–5 % activity of Factor VIII) and severe (<1 % activity) usually become symptomatic after minor surgical procedures or spontaneously bleed. Approximately 70–80 % of bleeding episodes result in severe bleeding in the joints. Progressive Haemophilia joint arthritis is the most important long-time complication.
The first successful blood transfusion was performed post-World War II on an 11-year-old boy and thereafter increased access of Haemophiliac patients to blood or plasma transfusions improved their life- expectancy to 30 years of age.
The life expectancy of Haemophiliacs improved further when Judith G. Pool in 1964 discovered a frozen fraction of plasma contained proportionally greater quantities of Factor VIII. In the 1970s. Nilsson and Ahlberg in Sweden pioneered the regular administration of Factor VIII in a prophylactic study, and life expectancy was increased to 68 years of age. Infusion and transfusion of plasma derivatives were not safe, and complications started to appear soon thereafter as they were obtained by donations from poor people, paid for donating, and these people had a higher frequency of infectious agents in their blood.
The Human Immunodeficiency Virus (HIV) appeared in the 1980’s, and the first haemophilic HIV patient in the US was reported in 1982. In the US the HIV incidence increased to 60 cases per million in 1990. HIV accounted for 25% of deaths in Haemophiliacs in the 1990s in Netherlands. Two years later it was discovered that 60 % of the US haemophilic patients, and 80 % of all patients ever treated with clotting factor concentrates were already infected with hepatitis C.
The genetic sequence of Factor VIII gene was elucidated in mid-1980 and this led to the production of recombinant Factor VIII (rFactor VIII). The new rFactor VIII was expressed in culture and the first patient treated was in 1987. Thereafter, no donations were required as the use of the recombinant rFactor VIII became the treatment of choice. Since 1985 there were no further reports of viral transmission linked to the use of rFactor VIII in the developed world. These recombinant clotting factors have increased the life expectancy of all Haemophiliacs worldwide. The life expectancy for a mild to moderate Haemophiliac is 70 years of age, whereas for severe cases of Haemophilia, it is estimated to be at least 15 years less.
Since the 1990s risk of blood-borne infections has been controlled with the use of recombinant replacement therapy, as well as with the introduction of more sensitive immunoassays for the serological markers associated with transfusion-transmitted viruses (TTVs). A new complication has emerged in Haemophilia, that of the development of inhibitors (a neutralising immunoglobulin directly acting against Factor VIII) which is now the most frequent and serious complication. Academics are now focused on comparing different treatment options and their association with the emergence of these antibodies. Since 2000, researchers have focused their efforts on the costs and cost-effectiveness of long-term treatment.
There is currently no cure for Haemophilia.
Currently Haemophilia treatment for severe cases is regular injection of clotting factor. The cost of treatment is extremely expensive, approximately $400,000 per patient (R7,2 million per patient) per year and the majority of patients in the world with the disorder don’t have access to this treatment. In addition, about a third of patients develop antibodies to the treatment.
Haemophilia is a monogenic disorder, has a broad therapeutic window, has very good animal models, and is therefore ideal for gene and/or cell therapy. Gene therapy using adeno-associated virus (AAV) vector is an option and has shown promise for long-term therapy, but AAV-vector based approaches carry with them problems, including possible tissue damage and immunogenicity. The clotting factors are mainly produced in the liver, so liver transplantation is an alternative long-term treatment option. However, there is a scarcity of donor organs and the need for constant immunosuppression represents a major drawback. A number of these gene therapy candidates for Haemophilia A, such as SB-525 by Sangamo Therapeutics and Pfizer; AMT-180 by uniQure; and BioMarin’s valoctocogene roxaparvovec, or BMN 270, are under development and clinical in testing. All of them are based on an adeno-associated virus (AAV) vector, to deliver a functional version of the F8 gene to the patient’s cells. The risks associated with AAV-vector-based therapy are far from elucidated and carry many risks.
Therefore, being able to cure haemophilia with stem cell transplants would be a significant breakthrough.
The first research strategy would be to engineer mesenchymal stem cells (MSCs), a type of adult stem cell so that they produce high levels of factor VIII. The cells, acting as a carrier for the gene, would then be transplanted into the patient. Even though the approach might not be successful at curing the disease, it would at least solve the antibody problem so that the current treatment would be effective.
In some instances, haematopoietic stem cell transplant (HSCT) has become an emerging therapy approach for Haemophilia patients.
In the first case where a boy underwent allogeneic (from a donor) HSCT at age 4, the boy presented with increasing bleeding symptoms and prolonged PTT. He was eventually diagnosed with mild Haemophilia A with a residual FVIII-activity of 18 percent in the absence of FVIII-inhibitors. Additional examinations revealed MDS-RAEB (myelodysplastic syndrome-refractory anaemia with excess blasts) and this leads to low levels of any type of blood cell. After HSCT, the FVIII activity spontaneously increased to a maximal level of 45 percent, remained elevated for four weeks, but ultimately declined to pre-HSCT levels two months later. The child’s recovery post-procedure went well, with no associated toxicity or immune system rejection. At the last follow-up of the boy’s condition, his factor VIII activity was at 19.6% and he did not have any bleeding symptoms. He was not cured but remained in a stable condition.
In the first testing of this treatment in animals, the researchers used stem cells from the father’s bone marrow, which were engineered to produce high levels of factor VIII. MSCs were selected because they are home to sites of injury or inflammation. In two of the treated animals, the cells homed to the sites of injury and stopped the bleeding and in addition, all spontaneous bleeding events ceased. The existing joint damage was completely reversed, thus improving the normal posture and gait of the crippled animals, and they resumed normal activity. Currently, scientists are working to find better ways of administering cells and to understand a paradox of the treatment—while the stem cells were able to stop the bleeding, the treatment induced an immune response in the animals.
Because the gene for Factor VIII is enormous, 26 exons, it cannot readily be delivered by a virus for genetic engineering purposes, some scientists have tried truncating the gene. Stem cells can overcome this bottleneck. Sinusoidal endothelial cells in the liver are the main producers of Factor VIII. Thus, using stem cells that can differentiate into endothelial cells can be a great solution for Haemophilia overall. Bone marrow has a similar capacity to transdifferentiate into sinusoidal endothelial cells, which can compensate for the deficiency of factor VIII. They even have the potential to treat chronic liver failure and liver injury.
Thus, researchers at the Boston Children’s Hospital’s Department of Cardiac Surgery laboratory came up with a strategy to test this use of stem cells in Haemophilia. They reprogrammed the epithelial cells obtained from urine samples of Haemophiliacs into induced pluripotent stem cells. They used gene-editing on the iPS cells, inserting multiple copies of the normal gene for factor VIII using a so-called piggyBac transposon system. Finally, they used the edited iPS cells to create large quantities of endothelial cells, which line blood vessels and naturally secrete factor VIII protein.
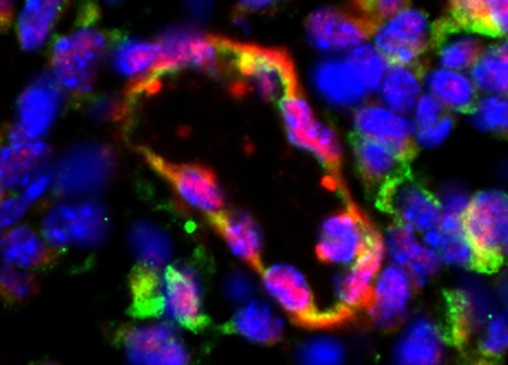
A bioengineered blood vessel secreting factor VIII (shown in green), seven days after implantation of treated human cells in mice with Haemophilia.
Courtesy of Melero-Martin Lab/Boston Children’s Hospital.
A Factor VIII for Haemophilia A, named ET-3 has been purified and demonstrated to be indistinguishable and superior to human Factor VIII with respect to intracellular processing, activation and stability, and in vivo efficacy. ET-3 specific activity is approximately 50% greater for the engineered protein, its half-life following activation is approximately 3-fold longer, and it engages the unfolded protein response to a lesser extent than human Factor VIII. Transplant of ET-3 lentiviral-modified CD34+ cells into mice resulted in ET-3 expression in all mice comparable with normal levels. The goal of this project remains to obtain clinical approval for a haematopoietic stem cell transplant gene therapy clinical trial for haemophilia A.
Another group used a combination of ex vivo-engineered stem cells for their approach. First, they collected placenta-derived mesenchymal stromal cells (PMSCs) and endothelial colony-forming cells (ECFCs) from discarded human term placenta and ECFCs from umbilical cord blood, respectively. These cells were then genetically engineered with a version of FVIII to express a functional Factor VIII, using lentiviral-based gene therapy. The genetically modified cells were transplanted alone or in combination into immune-deficient mice to check which one of the regimens allowed cells to last longer inside the body. The results showed that the co-transplant of PMSCs and ECFCs resulted in the best and longer transplants, stably producing a functional Factor VIII inside the mice’s bodies over at least six months. In addition, the transplant was more successful if performed a few days after birth, compared with transplants in adults.
Haemophilia B on the other hand can be used in viral genetic delivery because it is a smaller gene, it has 8 exons. Salk Institute researchers have combined CRISPR-Cas9 gene editing with stem cell technology to make an autologous cell therapy for the genetic blood clotting disorder Haemophilia B. In mice, in vivo tests showed that gene-edited, stem cell–derived liver cells were viable and functional in Haemophiliac mice for nearly a year, after a single injection.
Other approaches to stem cell therapy have been tested at the Salk Institute, using cells from donor livers or derived from autologous stem cells. Three major sources of hepatocytes exist, heterologous cadaveric hepatocytes, pluripotent stem cell-derived hepatic-like cells (HLCs), derived from embryonic stem cells (ESCs) or induced pluripotent stem cells (iPSCs), and induced HLCs (Heps) derived by direct reprogramming of fibroblasts into HLCs. These sources have their own respective advantages and disadvantages.
In order to test two different approaches to long-term cell therapy, the Salk Institute team first developed a new, quadruple knockout mouse model of Haemophilia B that was able to accommodate the engraftment and expansion of human hepatocytes (hHeps).
They first transplanted cadaveric, cryopreserved induced pluripotent stem cell-derived hepatic-like cells, directly into the spleens of the Haemophiliac animals. These transplanted cells readily engrafted and remained healthy, functional, and non-tumorigenic. They have tested hepatocytes from multiple donors and sources and have not seen any adverse reactions in the more than 40 animals tested.
As an alternative to using heterologous donor hepatocytes, the Salk Institute team developed an approach based on the use of patients’ own, gene-corrected, and in vitro–differentiated cells. The aim was to generate hepatocyte-like cells (HLCs) from Factor IX gene-corrected iPSCs derived from peripheral blood-derived mononuclear cells (PBMCs) from Haemophiliac patients. The outcomes were as good as with the donor HLCs. The only drawback however was engraftment of these cells was not as good as in the cadaveric study. Encouragingly, data from prior studies of severe Haemophilia patients have suggested that low levels of 15% to 20% of Factor IX levels are sufficient to stop joint bleeding and might be therapeutically relevant.
The researchers concluded that the major benefits of the autologous cell therapy approach include the ability of IPSCs to support homology-directed repair recombination and gene editing. Additionally, because the cell therapy is derived from the patient’s own cells, there should be no risk of an immune reaction or the need for long-term immunosuppressive drugs.
In light of the recent findings of these different techniques of stem cell transplantation in Haemophilia patients, these promising results show that genetically engineered stem cells can potentially achieve stable, long-term engraftment in Haemophilia patients.
An efficient prognostic test for preeclampsia would enable early diagnosis, directed observations, and timely delivery; however, currently these options are restricted. In the last 2 years first-trimester screening algorithm was published after development and validation to predict preterm preeclampsia, with poor utility for term disease, where the greatest burden lies. Biomarkers such as sFlt-1 and placental growth factor are also currently being used clinically in cases of presumed preterm preeclampsia; their elevated negative predictive value facilitates confident exclusion of disease in women with normal results, but the sensitivity is modest. There has been a collaborative attempt to detect possible novel biomarkers that might increase predictive value. These largely originate from organs involved in preeclampsia’s pathogenesis, including placental, cardiovascular, and urinary biomarkers. A review of these biomarkers was published in December 2021 (2).
These two above-mentioned reviews highlight the research in PE over the past decades and with this summary, we wish to highlight novel findings related to stem cells and possible therapeutic applications that have emerged over the past 2 years.
Fetal microchimerism (FMc) in PE
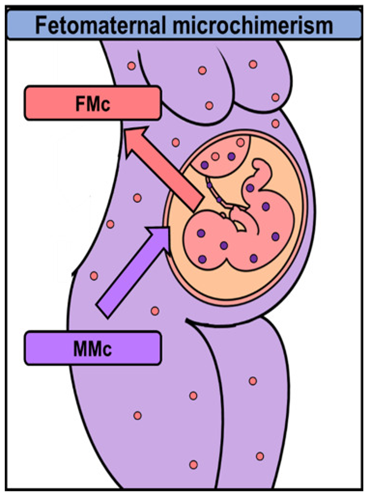
After almost forty years of study, the biological role of fetal microchimerism (FMc) remains enigmatic. Transmission of fetal cells to the mother begins soon after implantation and increases with gestational age. Feto-maternal microchimerism (FMM) on the other hand, involves bidirectional cross-placental trafficking during pregnancy, leading to a microchimeric state that can persist for years. In this way, a pregnant woman will harbour cells from her mother, as well as cells from her child.
Fetal microchimerism (FMc) is present as undifferentiated or differentiated cells throughout the maternal tissues. FMc has been linked to autoimmune tolerance and tissue repair but also with autoimmune diseases and cancer, creating the probability that they exercise numerous and opposing effects in a mother’s body. Evidence indicates that different pregnancy and birth complications, caesarean sections, antepartum hemorrhages, and PE, might alter the functional fate of FMc.
Figure 1: Fetal cells (pink circles) traffic into and set up in the maternal organism (FMc). Maternal cells (purple circles) also traffic into and remain in the fetal body (MMc).
Bi-directional cell trafficking between mother and fetus is also modified in PE and has been proposed to contribute to the underlying aetiology. The fundamental mechanism whereby the host immune system is controlled is uncertain, but seems to entail HLA class II molecules, Couples that have a high level of HLA class II compatibility have a higher risk of PE. Since pregnant women with PE exhibit significantly lower levels of maternally-derived micro-chimerism, the question arises whether preeclampsia and post-partum development of autoimmune conditions occur due to the failure of the grandmothers’ cells to sufficiently regulate an unsuitable micro-chimeric pattern.
Current evidence indicates that FMc within the maternal peripheral blood mononuclear cell (PBMC) compartment, which is characterised by incomplete clearance, immune competence, and pluripotency, may underpin the maternal immune dysfunction seen in PE and may lead to long-term persistence after PE pregnancy. This FMc within the maternal circulation can permanently persist decades after pregnancy and is known to arise at greater frequency in PE, which can potentially affect local and systemic immune programming.
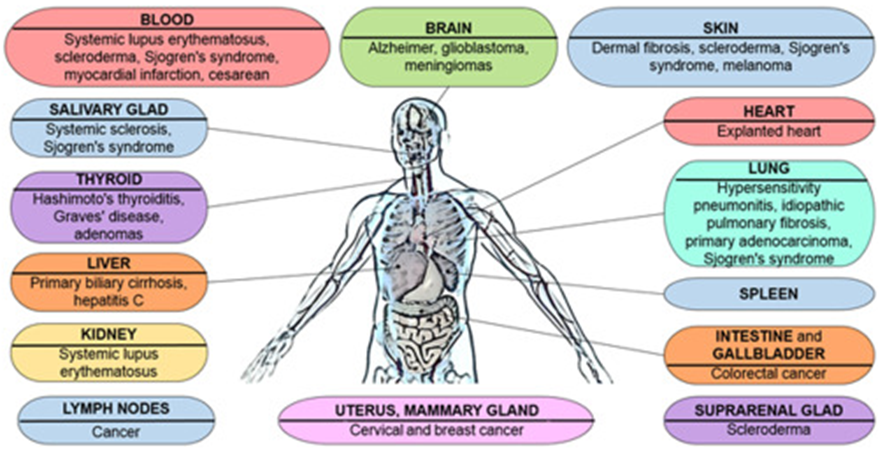
Figure 2. Representation of the different organs where FMc have been localized in humans and the diseases associated. (Blanca Cómitre-Mariano, et al. Feto-maternal microchimerism: Memories from pregnancy, iScience, Volume 25, Issue 1, 2022)
In a recent study conducted by a group at the Department of Obstetrics and Gynaecology, University of Washington, they found a significant increase in FMc concentration in immune cell subsets in PE cases compared to controls, primarily in B cell, and NK cell lymphocyte populations. There was no substantial difference in FMc frequency or concentration within the stem cell population between PE and controls (3).
Regarding the role of natural killer cells (NKCs) in pregnancy. NKCs are among the most abundant immune cells in the uterus during the first trimester of pregnancy, but their numbers decrease substantially after the placenta forms. A new study, by scientists in China, discovered that a specific subset of NKCs in the human uterine lining secretes growth-promoting factors called pleiotrophin and osteoglycin, which participate in extensive developmental processes. This subset of cells made up a smaller proportion of natural killer cells in the uterine lining of patients who experienced recurrent spontaneous abortion (42%) compared to healthy females (81%). These results suggest that inadequate secretion of growth-promoting factors by a particular subset of natural killer cells may be responsible for restricted fetal development in humans. The researchers identified a specific subset of uterine natural killer cells that secrete growth-promoting factors in humans and mice, and further demonstrated that transfer of these cells can reverse impaired fetal growth in pregnant mice (4).
Mesenchymal stem cells (MSCs) in PE
Mesenchymal stem cells (MSCs) have earned increasing attention due to their easy cultivation, low immunogenicity and expansion in vitro. MSCs are the most extensively studied stem cells currently being investigated for treatment of many diseases.
MSCs act as injury sensors and are recruited to the injury site in reaction to stress signals (inflammation, hypoxia, and the like) and then engage in tissue repair. Besides this, MSCs react to growth signals and take part in programmed tissue development, MSCs replace injured tissue by both differentiating into tissue cells directly and secreting trophic cytokines to promote the proliferation of tissue cells indirectly. Likewise, inflammatory signals can also encourage MSCs to develop an immunosuppressive phenotype thus inhibiting inflammation/immune triggering in injured tissue. MSCs-assisted angiogenesis facilitates damaged tissue to restore the vascular system and regain blood supply. More intriguingly, MSCs express low levels of HLA Class I and II and high levels of HLA-G, therefore, MSCs show relative low immunogenicity after allotransplantation. Paracrine nutrition, anti-inflammation/immune-modulation, multi-differentiation, damage sensing and low immunogenicity characteristics have made MSCs transplantation a potent therapy in tissue repair and systematic inflammation/immune disorders.
In recent years, MSCs or their secreted cargo (exosomes) have been studied in various animal models of PE and showed encouraging result, which inspired further investigations into the therapeutic effects and mechanisms of MSC-based therapies in PE.
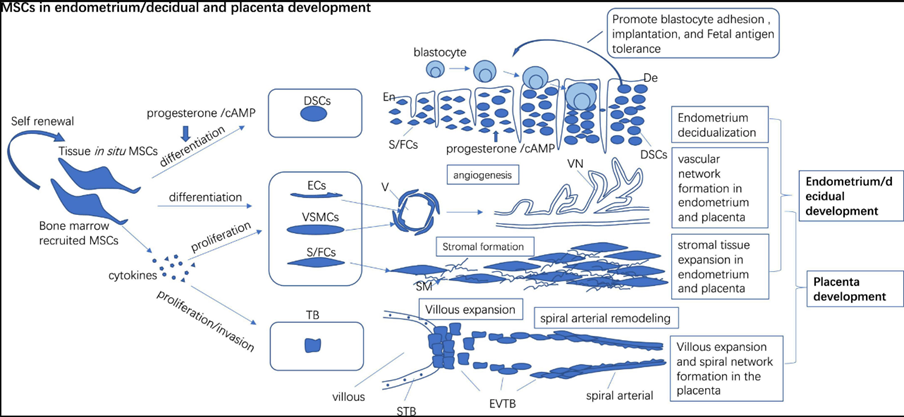
Figure 3. In situ and bone marrow recruited MSCs to participate in endometrium/decidual and placenta development by direct differentiating into endothelial, vascular smooth muscle cells, and stromal cells to form vascular and stromal tissue de novo and promote the proliferation of preexisting vascular cells and the stromal cells to build the vascular network and stromal in tissue. Progesterone/cAMP induces decidual stromal cell (DSCs) like changes in MSCs and expresses high levels of receptive markers which may promote blastocyte adhesion, implantation, and fetal antigen tolerance. MSCs secret multiple cytokines to promote proliferation and invasion of trophoblast (TB) which may foster villous expansion and maternal spinal arterial remodeling. (S Jin. Et al. The pathological and therapeutic roles of mesenchymal stem cells in preeclampsia. Front. Med., 28 July 2022.Volume 9 – 2022 | https://doi.org/10.3389/fmed.2022.923334)
Remodelling of the uterine vasculature in PE
In the past few decades researchers have investigated the role of remodelling of the uterine vasculature as one of the underlying mechanisms of PE, intrauterine growth restrictions and preterm births. It is well known that the remodelling of the uterine vasculature by invasive extravillous trophoblasts (EVTs) is a vital part of human placentation. This remodelling involves alterations in the arterial system from a high-pressure low flow system to a low-pressure high flow system. These changes results in significant structural and functional changes in large and small arteries and veins in the arterial walls. Insufficient EVT penetration can lead to severe obstetrical complications like PE, intrauterine growth restriction, and preterm birth.
A specific transcription factor has been extensively studied in this remodelling process, Glial cells missing-1 (GCM1) is crucial for proper placentation in mice and is highly expressed in human syncytiotrophoblast (ST) and EVTs. GCM1 is classically believed as a master regulator of ST formation, but little is known about its involvement in the growth and function of EVTs. Researchers have shown that GCM1 is highly expressed in human trophoblast stem (TS) cells differentiated into either ST or EVTs. RNA sequencing analysis of GCM1-deficient TS cells revealed downregulation of EVT-associated genes and enrichment in transcripts related to WNT signalling, which was linked to decreased expression of the EVT master regulator ASCL2 and the WNT antagonist NOTUM. Therefore, this research highlighted an essential role of GCM1 during ST and EVT development and suggest that GCM1 regulates differentiation of human TS cells into EVTs by inducing expression of ASCL2 and NOTUM (5).
The same research group further identified a mitochondrial creatine kinase 1 (CKMT1) as a key GCM1 target crucial for syncytiotrophoblast differentiation and reveal decreased CKMT1 expression in PE.
They found that the induction efficiency of cytotrophoblast is determined by functional antagonism of the placental transcription factor GCM1 and the stemness regulator ΔNp63α. ΔNp63α reduces GCM1 transcriptional activity, whereas GCM1 inhibits ΔNp63α oligomerization and autoregulation. EGF/CASVY cocktail activated ΔNp63α, thereby partially inhibiting GCM1 activity and reverting term cytotrophoblasts into stem cells (6). By applying hypoxia condition, they reduced GCM1 activity and successfully induce term cytotrophoblasts into TS cells. They found that trophoblast stem (TS) term cells can easily be established from every individual’s placenta and propagated for lifetime storage as an abundant source of stem cells, which may offer enormous potential for autologous cell therapy.
Exosomes in PE
It is well known that poor placentation secretes exosomes as well as anti-angiogenic factors that results in increased immune responsiveness, proinflammatory cytokines and anti-angiogenic factors. On the other hand, anti-inflammatory cytokines and pro-angiogenic factors are decreased. Preeclampsia (PE)-specific exosomes derived from damaged trophoblasts are secreted and may transport RNA, DNA, and proteins to distant maternal organs, causing multiple-organ failure, especially due to endothelial dysfunction. Evidence suggests that the pathogenesis of PE may be ameliorated by the immunosuppressive and anti-inflammatory effects of mesenchymal stem cell (MSC)-derived exosomes (7).
Another group investigating during transfection experiments the role of human umbilical cord mesenchymal stem cell (hucMSC)-derived exosomes in PE, by using these exosomes transmitting microRNA-342-5p (miR-342-5p) by targeting programmed cell death 4 (PDCD4). They concluded in their study that the HucMSC-Exo carrying elevated miR-342-5p prevents the development of PE in a rat model through downregulating of the gene PDCD4. This study illustrates the way that ex vivo manipulation of these exosomes could aid in developing therapeutic strategies for PE in future (8).
Therefore, exosomes may be involved in the pathogenesis of PE and have great potential for the treatment of this disease. PE pathogenesis could be improved or prevented by inhibiting exosome effects or preventing their binding to target organs. By first examining the effects of exosomes released from the preeclamptic placenta on various organs by searching for proteins, RNA, and DNA in the exosomes. Exosomes could be used as markers to predict the onset of PE and to follow the course of this disease. In 2012 Marleau, suggested that the anticancer effects of molecular targeted drugs could be enhanced by removing exosomes from the circulating blood via hemodialysis. This approach may also be used to treat PE via the removal of STB EVs. The use of various exosome-based methods may aid the identification of the best solution for PE prevention and treatment (9).
Conclusion
Preeclampsia remains one of the most serious pregnancy complications with a substantial vestige of both maternal and perinatal morbidity. Early detection improves outcomes, yet at present there is no reliable screening test to predict its development – especially at term gestations where the greatest burden of disease exists.
Many potential biomarkers have been discovered through investigative studies using samples from well-known disease. These studies have produced hypotheses for potential biomarkers, with less focus on prediction. It is possible that combining biomarkers derived from multiple organ and cellular sources may yield the best predictive performance. Utilising large prospective cohort collections in unselected populations provides the best avenue for discovering novel biomarkers, but these markers – or combinations – must be rigorously validated in external cohorts to ensure they achieve their potential to improve outcomes for pregnant mothers and their babies. Thus the development of multiple biomarkers with exact test outcomes will offer a multi- dimensional focus to complete the antenatal and postnatal care of PE. The main intent hereof is to provide rapid bedside prediction of women with suspected PE. Numerous biochemical factors in combination with superior therapeutic methodologies, which have been shown to be valuable and expandable into widespread clinical practice, will be incorporated into the management standard of patients with suspected or confirmed PE over the coming years. Currently there is no therapy to reverse the process once started and although various stem cell therapeutic approaches have shown improved outcomes in PE, these treatments are still in the investigative phase and not yet approved. However, these stem cell therapies might prove invaluable in future by virtue of their mode of action, whereby they act as sensors and are recruited to the site of injury in reaction to stress signals, thus effecting their “healing” principles at the exact sites of inflammation, hypoxia, and the like, in accordance with the multifactorial mode of pathogenesis of PE.
Tissue engineering is the application of biologically compatible scaffolds that are implanted in the body at the site where new tissue is to be formed. The scaffold might be in the geometric shape of the tissue that needs to be formed, the scaffold might attract cells or cells will be implanted and the outcome is new tissue in the shape desired.
2. Cellular Therapies
Stem cells are important for the body to repair itself and many millions of adult stem cells are found in every human. These cellular therapies involve the use of adult stem cells that are injected at the site of diseased or damaged tissue, where the rebuilding of the tissue is possible under the right stimuli. These adult cells can be collected from blood, fat, bone marrow, dental pulp, skeletal muscle, and other sources. Cord blood is one of the most unique and potent sources of stem cells currently in use.
3. Medical Devices and Artificial Organs
In cases where an organ fails, the main clinical approach is to transplant a substitute organ from a donor. One of the major challenges are the availability of donor organs and the requirement that the donor takes immunosuppression drugs—which have significant side effects and risks. A novel strategy that has emerged is the 3-D printing of organs. In this way, the stem cells that build the new organ are manipulated to form the tissue of the specific organ and these cells will populate a 3-D scaffold of the organ. These stem cells can be engineered from the same patient’s cells and thereby any organ rejection will be eliminated.
Studies have shown promising results in treating burns, heart disease, trauma and other diseases.
To quote the Biopharma Reporter:
“We are on track for a watershed year for approvals of new regenerative medicine and advanced therapies globally. Decisions are expected on 18 regenerative medicine products across 6 geographies, with 10 of these on products that have never been previously approved in any geography – meaning new product approvals could exceed the record of nine set in 2016.”
There are currently 2,600 clinical trials ongoing worldwide in this sector, of these 1,320 are industry-sponsored and an additional 1,328 non-industry sponsored. There are 243 trials in Phase 3, including 1158 industry-sponsored trials and 85 trials sponsored by academics, the government and other institutions. The late-stage products are being tested for instance in diabetic neuropathy, heart failure, rare genetic diseases, and neuromuscular diseases.
The biggest buzzword in the industry is “off-the-shelf” therapies, which are easily accessible. Therefore, as the field continues to grow, developers are seeking to work more closely with regulators to set improved standards. All these developments in the field of regenerative medicine across a broad scope of medical disciplines will ultimately aid in new solutions to expand and sustain optimal health and quality of life.
Some factors increase the risk of developing severe disease in pregnancy. These include pre-existing diabetes, high blood pressure, obesity, and being over the age of 35. People of Black, Asian and Hispanic origin have also shown an increased risk to severe disease.
Pregnant women who develop severe disease will have a greater chance of needing admission to ICU and a greater need for mechanical ventilation. There is an increased risk of developing blood clots as well as an increased risk of premature birth and fetal loss, nevertheless, the absolute number of these complications remains small. Needless to say, the vast majority of women who get infected with COVID will have mild disease.
Mother-to-baby transmission is uncommon and most infected babies have mild symptoms or no symptoms at all. The method of delivery does not seem to affect the infection rate in the baby. It is thus most likely that if the mother has COVID in her pregnancy, the baby will not be infected.
Vaccination is advised in all women contemplating pregnancy, as there is no current evidence linking the vaccine to infertility. If you are pregnant, vaccination is strongly recommended. There is no evidence that the vaccine could harm your baby but as a precaution in South Africa, it is suggested that you vaccinate after 12 weeks. If you get the vaccine in early pregnancy, before you know you are pregnant, there is no evidence to suggest that the baby will be harmed. The choice lies with you as parents, whether you vaccinate before you know you are pregnant, after the first trimester, or even soon after birth, there is no indication that it could harm your baby.
There is however a small increased risk of severe disease in pregnancy, especially if the known high-risk co-morbidities like diabetes, obesity, and high blood pressure are present as well. Be extra careful about wearing a mask, social distancing, washing hands, and disinfecting, as well as avoiding crowds and gatherings.
The South African Society of Obstetricians and Gynaecologists (SASOG) has a website with very useful and regularly updated information on COVID in pregnancy. Search for SASOG, and the section on COVID in pregnancy will be easy to find.
The Royal College of Obstetricians and Gynaecologists (RCOG) also has a patient information section on their website covering a large number of topics. The section on COVID also contains links to other useful sites. Search RCOG and look for “COVID in pregnancy”.”
Mesenchymal stem cells (MSCs) are the stem cells that might be the most encouraging treatment for SARS-CoV-2 infections. The main factor in treating SARS-CoV-2 infection lies in the management of the cytokine storm in the lungs, therefore MSCs are suitable for this since their main mode of action is through their immunomodulatory, anti-inflammatory properties, as well as their ability to restore and remodel the lungs.
Since the start of the pandemic, more than 17 clinical trials evaluating the benefits of MSCs for the treatment of COVID-19 are underway. In previous years before the pandemic, the safety and efficacy of MSCs have been well established based on the completion of other clinical trials in lung diseases such as acute respiratory distress syndrome (ARDS) (Chen J, et al. 2020), bronchopulmonary dysplasia (Namba 2020), cardiovascular diseases (Kim et al. 2015), diabetes (Thakkar et al. 20150, and spinal cord injury (Xu and yang, 2019).
MSCs have been investigated as early as 2013 and 2015 for the treatment of ARDS and have shown the capacity to stimulate repair in the distal ends of the lungs.
In a comprehensive study of the clinical trials using MSCs for the treatment of ARDS, 2691 studies were reviewed. The MSCs were from various sources but were all allogeneic from either bone marrow, umbilical cord, menstrual blood, adipose tissue, or unreported sources. Overall, the patients showed better survival, no severe side effects. The patients also showed improved lung scans, lung functionality, and improved inflammatory marker levels.
All these studies concluded that ARDS patients showed low risk, reduced risk of death, and improvement in lung functionality using MSC treatment. The MSC treatment also eased the clinical symptoms leading to ARDS.
It is therefore believed that evidence suggests a favourable benefit of using MSC therapy for COVID‐19 patients. However, it is suggested that larger clinical trials that follow the same protocol should be used to standardise the treatment of ARDS.
The ability to immediately bank these samples in a family (private) stem cell bank, for future use by the child (donor) or a sibling.
Cord blood stored in ‘public’ cord blood banks are made available for use by non-related individuals. These cord blood stem cells can be made available for transplant, without delay, and are more ‘naïve’ than the other sources of blood-forming stem cells i.e., bone marrow (BM) and peripheral blood stem cells (PBSCs).
Defining Graft-versus-Host Disease
The day-to-day task of a person’s immune system is to protect it from foreign invaders, be it a bacteria, virus or other organisms or cells that are not identified as ‘self’.
When a person needs a stem cell transplant, a donor, who is a match for the specific patient, must be found. This is what we call Human Leukocyte Antigen (HLA) matching or, in non-medical terms, “flags” that the immune system must look at to determine if something is an invader. With a stem cell transplant, the recipient will receive donor stem cells and these cells will form new blood as well as an immune system in the recipient.
Higher levels of differences of human leukocyte antigen (HLA) matching can be tolerated with CBT, confers a potential advantage. Also, some studies have shown a lower incidence of graft-versus-host disease (GvHD) with CBTs compared to bone marrow and peripheral blood stem cell transplants.
These features make a cord blood transplant as a potentially important option in patients from diverse, cultural and ethnic backgrounds as, for these patients, it can often be challenging to locate a matched unrelated donor (MUD).
With a stem cell transplant, even after HLA matching, the patient/recipient’s body will still see small differences between the new developing immune system and other cells in their body. Therefore, the recipient’s “new” immune system may harm some of the recipient’s cells because they are seen as “different”. This immune attack (on the recipient) is called Graft versus Host Disease (GvHD). The word ‘graft’ referring to the donor’s cells, and the ‘host’, to the patient (recipient).
The good of Graft-vs-Host-Disease
GvHD can have a ‘good’ aspect as it indicates that the recipient’s new immune system is working and is likely to be attacking any remaining or returning disease. This type of immune response is called ‘graft versus leukaemia effect’ or ‘graft versus tumour effect’. However, extreme GvHD can cause undesirable problems and side effects which is life threatening.
The not-so good
GvHD is complex and cannot be predicted. Approximately, 30-40% % of transplant recipients will show signs of GvHD. In certain cases, it is mild but, in severe cases, may be life-threatening.
GvHD can be classified as the following:
Acute: occurring within the first 100 days after transplant
Chronic: usually occurring after 100 days and
Overlap: having features of both acute and chronic GvHD.
GvHD affects organs such as the skin, liver, and gastrointestinal system.
It usually requires a fine balance of medication to keep the disease under control. Treatment includes localised and/or systemic steroids or immunosuppressive medication. In some cases, acute or chronic GvHD cannot be controlled with these medications and further treatment, such as extracorporeal photopheresis (ECP) (where the white blood cells that cause GvHD are destroyed with medication and ultra-violet (UV) light, is required).
Several strategies exist to further improve outcomes in CBT and minimise GvHD even further:
The use of double CBT from unrelated donors
The use of HLA-identical sibling CBT
The use of a combination of UCB and bone marrow from the same sibling,
The use of higher cell doses in conjunction with microenvironmental factors and, for example, the combined use of mesenchymal stem cells.
These strategies are designed to enhance the ‘homing’ and engraftment of the transplanted cells and improve success rates overall.
Final words
Parents should consider storing their baby’s stem cells at birth, which would give the Transplant Team an option should a stem cell transplant be needed.
Did you know
Since the first cord blood transplant in 1988, more than 40,000 CBTs have been performed, worldwide, over the past three decades.
We use cookies and similar technologies to improve your experience on our website.